You’ve been there before, probably saying it a hundred times. You might have said gently, then firmly and through tears. Every time it made things worse: a slammed door, thrown object, or a screaming match that left everyone shaking and exhausted. You’re not doing it wrong. “Calm down” doesn’t work because it can’t work. Especially for a teen who has learned that word is not safe.
The clinical team at BlueRock Behavioral Health can help turn panic into peace when a teenager is in the grip of emotional dysregulation and anxiety.
The Cleveland Clinic says emotional dysregulation is the inability to manage the intensity, duration, or expression of emotional responses in ways that fit the situation. In teenagers, it shows up as explosive outbursts, rapid emotional shifts, prolonged shutdowns, or reactions that seem wildly out of proportion to what triggered them. It’s not defiance or manipulation. It’s a nervous system that hasn’t yet learned how to regulate itself.
Key Takeaways
- Emotional dysregulation is a nervous system issue, not a character flaw, in your teen or in you.
- The adolescent brain is structurally wired for big emotional reactions; this is normal, but it can become a crisis without the right support.
- In-the-moment co-regulation and sensory grounding can reduce intensity, but they don’t treat the underlying cause.
- If home strategies and outpatient therapy aren’t holding, a higher level of structured care may be what your teen actually needs.
- Residential treatment in Western NC, like the program at BlueRock, is accessible to families on Medicaid and commercial insurance, and includes on-site schooling so teens don’t fall behind.
Quick Self-Check: Is What You’re Seeing Emotional Dysregulation?
Answer yes or no:
- Does my teen’s reaction seem far bigger than what caused it?
- Do they struggle to calm down even after the immediate trigger is gone?
- Do you find yourself walking on eggshells to avoid a meltdown?
- Has their mood become unpredictable in ways that affect the whole household?
- Do they seem unable to use coping skills they’ve been taught, even ones that used to help?
- Has the frequency or intensity of outbursts increased over the past few months?
- Have school refusal, self-harm, or substance use appeared alongside the emotional escalation?
If you answered yes to three or more of these, you’re not dealing with typical teen moodiness. You’re dealing with something that deserves real clinical attention.
Why Adolescent Brains Are Wired for Big Reactions
The teenage brain is genuinely unfinished. The prefrontal cortex (the part responsible for impulse control, emotional braking, and thinking before acting) doesn’t fully develop until the mid-twenties. What is fully developed, and running hot, is the amygdala: the threat-detection center.
This means adolescents are working with a fire alarm that’s sensitive and a sprinkler system that’s still being installed. Big feelings come fast, and the mental equipment to slow them down is still years from completion. It’s a biological reality that shapes how any effective treatment needs to work.
For most teens, this imbalance smooths out with time and experience. For others, especially those who’ve experienced trauma or disrupted attachment, the wiring gets reinforced in ways that make dysregulation more severe and more frequent. Their nervous systems learned to stay on high alert, because at some point, that alert kept them safe.
The Role of Trauma and Attachment in Emotional Escalation
When a child grows up in an environment with inconsistent caregiving, chronic stress, abuse, or loss, their brain adapts. It becomes faster to perceive threat, quicker to activate a stress response, and slower to settle back down. These are survival adaptations.
A teen whose nervous system learned dysregulation in the context of unsafe attachment needs to experience safe, consistent, attuned connection to rewire. This is why lectures don’t work. Consequences rarely land. What actually moves the needle is a therapeutic relationship where a teen learns, slowly and repeatedly, that they won’t be abandoned or shamed when they fall apart.
This is also why the treatment model matters enormously. Approaches built on punishment, isolation, or coercion don’t help dysregulated teens. They reinforce the very neural pathways that created the problem.
Tools That Can Help Your Teen Reclaim Control
In-the-Moment Strategies (When the Storm Is Happening)
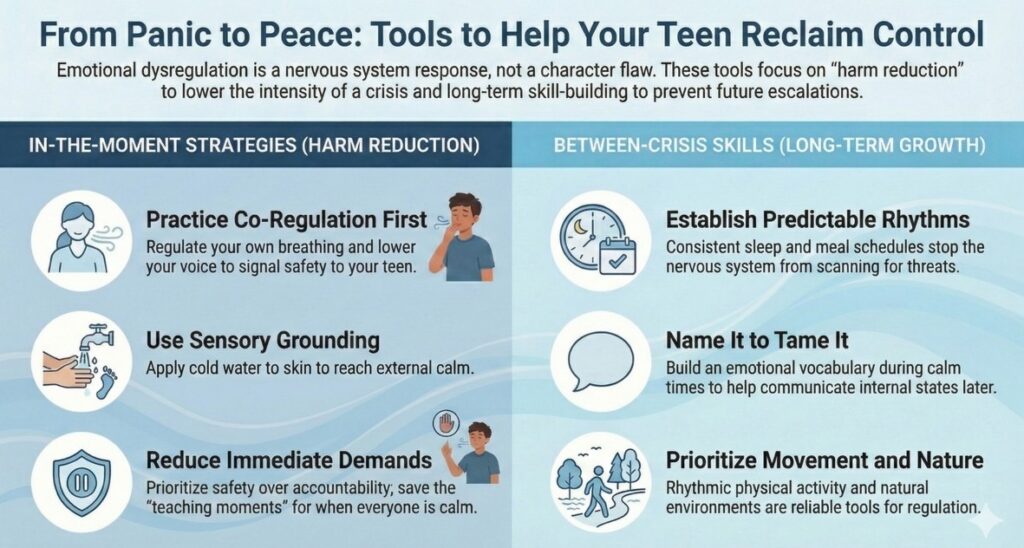
These aren’t cures. They’re harm reduction: ways to lower the temperature enough that everyone survives the moment.
Co-regulation first. Your teenager’s nervous system is looking for an external signal that things are okay. Before you try to reason with them, regulate yourself. Lower your voice. Slow your breathing. Reduce your physical size if you can; sit down, step back. You’re not rewarding the behavior. You’re communicating safety to a brain that’s in crisis.
Sensory grounding. When a teen is flooded, abstract language stops reaching them. What can reach them is physical sensation: cold water on the face or wrists, or standing barefoot on the floor and naming five things they can feel. These activate the body’s own regulation system by giving the nervous system something concrete to process.
Reduce demands, for now. In the middle of an escalation, this is not the moment for accountability conversations. Those can happen when everyone is calm. Right now, the goal is safe.
Know when to step back. Sometimes the most regulating thing you can do is say, quietly, “I’m here when you’re ready,” and then actually give them space. Not as punishment. As an invitation.
Between-Crisis Skills to Build Over Time
Predictable structure. Dysregulated teens do better when they know what’s coming. Predictable mealtimes, consistent sleep schedules, a stable daily rhythm: these aren’t boring, they’re regulating. The nervous system stops spending energy scanning for what’s next.
Name it to tame it. Help your teen build an emotional vocabulary over time, not in the moment. During calm stretches, talk about emotions: your own, characters in shows, people you know. The more words a teen has for internal states, the more capacity they develop to tolerate and communicate with them.
Movement and nature. Physical activity, especially rhythmic movement, is one of the most reliable regulation tools we have. Screens and sedentary isolation tend to amplify dysregulation; movement and natural environments tend to reduce it.
Your own support. This one gets skipped constantly. Parenting a teen in crisis is traumatic. You cannot co-regulate a dysregulated child if you are also dysregulated. Finding your own therapist, support group, or even just one other parent who gets it.
Residential Treatment for Teens in Western North Carolina
There’s a question underneath everything you’ve been reading here, and it might be time to say it plainly: What if this isn’t enough?
Home strategies can reduce intensity. Outpatient therapy can build skills. But some teens have needs that outpace what any one clinician, once a week, can address, and what any family, no matter how devoted, can hold.
When to Seek a Higher Level of Care: Key Signs Your Teen Needs More Support
Consider that your teen may need an increased level of care, such as teen residential treatment, if you observe the following signs:
- Escalating Outbursts and Crises: The frequency or intensity of emotional outbursts is increasing.
- Hospitalization and Relapse: Your teen has been psychiatrically hospitalized but returned home only to quickly deteriorate in the same environment.
- Self-Harm or Substance Use: Self-harming behaviors or substance use have appeared alongside the emotional escalation.
- School Refusal: School has stopped being a viable option due to their emotional state or behavioral challenges.
When home strategies and outpatient therapy are no longer effective, these indicators suggest that a more structured, intensive therapeutic environment is necessary to achieve lasting change.
Visit BlueRock’s contact us page to get connected with our admissions team by calling 828-845-8454, verify your insurance and ask any questions you may have about the support we offer.
Finding the Right Support for Your Teen in Western North Carolina
In Western North Carolina, families from Asheville, Hendersonville, and surrounding areas have access to a full spectrum of adolescent behavioral health services, including outpatient therapy, IOPs (Intensive Outpatient Programs), and PHPs (Partial Hospitalization Programs).
However, for teens who stabilize in these programs only to regress at home, residential treatment often becomes the necessary next step. It’s not a reflection of failure in earlier programs, but a recognition that the environment driving emotional dysregulation and crisis needs to change.
BlueRock Behavioral Health offers long-term residential treatment for adolescents on a 140-acre campus in the Blue Ridge foothills near Hendersonville.
Why BlueRock for Teen Mental Health Treatment?
- Duration and Depth: Programs typically last three to six months—enough time for deep, sustained change to occur.
- Clinical Model: The approach is attachment-based and trauma-informed, focusing on consistent, safe therapeutic relationships to help teens rewire their nervous systems.
- Integrated Academics: Bearwallow Academy, an on-site accredited school, ensures students continue learning and do not fall behind, preserving a vital part of their identity.
- Financial Accessibility: BlueRock accepts both Medicaid and commercial insurance and holds North Carolina Medicaid Level II certification. This allows working families in Henderson County, Buncombe County, and across the state to access quality care without having to choose between their teen’s health and financial stability.
BlueRock is a therapeutic community where teens learn to live differently—it provides safety and structure without the feel of a lockdown facility.
Frequently Asked Questions
What is emotional dysregulation in teenagers and how do I know if my child has it?
Emotional dysregulation in teenagers is a pattern of emotional responses (outbursts, shutdowns, rapid mood shifts) that are disproportionate to the trigger and difficult for the teen to manage or recover from on their own. Signs include explosive reactions to minor events, extended distress after an incident, and an inability to use coping skills even when they know them. It’s different from typical teenage moodiness in its intensity, frequency, and the way it disrupts daily life for everyone in the household.
What can I do at home when my teenager is having a behavioral crisis?
At the moment, prioritize safety and regulation over reason. Lower your own voice and body tension first; your teen’s nervous system is looking for external calm. Use sensory grounding techniques like cold water on the wrists or barefoot floor contact. Reduce demands until the storm passes, then have the accountability conversation later when everyone is calm. These tools reduce intensity; they don’t replace clinical treatment.
How do I know if my teen needs residential treatment instead of outpatient therapy?
Consider residential care if your teen has been through outpatient therapy without sustained improvement, has required psychiatric hospitalization and returned to the same situation, is engaging in self-harm or substance use alongside behavioral escalation, or has stopped being able to function at school. A confidential consultation with a treatment team, like the one at BlueRock, can help you think through where your family is and what level of care actually fits.
Will my teen fall behind in school if they go to a residential treatment program?
At BlueRock, academic continuity is built into the model. Bearwallow Academy, the on-site accredited school on campus, allows students to keep learning while receiving treatment, so the transition back to their home school is manageable rather than overwhelming. Falling behind doesn’t have to be part of the equation.
Does residential treatment for teens work if they’ve already tried outpatient therapy?
Yes, and in many cases, outpatient therapy not working is precisely why residential becomes the right next step. Outpatient care requires a teen to do therapeutic work, then return to the environment driving the dysregulation. Adolescent residential treatment program changes the environment itself, which allows the therapeutic work to actually take hold. Attachment-based, trauma-informed residential models show meaningful outcomes, especially when treatment lasts long enough to address underlying patterns.
Is residential teen treatment covered by Medicaid or commercial insurance in North Carolina?
BlueRock accepts both Medicaid and commercial insurance, and holds North Carolina Medicaid Level II certification as a therapeutic, short-term living environment for youth. Coverage specifics vary by plan; our team can help you verify benefits and understand what your family’s financial responsibility would look like before you make any decisions.
How long does residential treatment in North Carolina for adolescents typically last?
At BlueRock, residential stays typically run three to six months. That length is intentional: meaningful change in attachment patterns, trauma responses, and behavioral regulation takes time. Short-term stabilization may be enough to manage a crisis, but it rarely addresses what’s underneath. The teens who benefit most are those who have enough time in a stable, therapeutic environment to actually practice a different way of being.
What’s the difference between a residential treatment center and a psychiatric hospital for teens?
A psychiatric hospital focuses on stabilization: getting a teen safe during an acute crisis, usually over days or a few weeks. A residential treatment center like BlueRock is designed for longer-term, deeper therapeutic work in a community setting. For many families in Western NC, a hospital stay is the beginning of the road toward residential, not an alternative to it.
How to Get Started
Contact our admissions team at BlueRock at 828-845-8454. You can verify your insurance at our contact us page.
BlueRock Behavioral Health is located at 41 Heroes Way in Hendersonville, North Carolina.
Safety Resources and Helpful Links
If you or your teen are in immediate crisis, please reach out:
- SAMHSA National Helpline: 1-800-662-HELP (4357)
- 988 Suicide & Crisis Lifeline: Call or text 988
- The Cleveland Clinic: Emotional Dysregulation
- National Institute of Health: Emotional Dysregulation in Adolescents
- Stanford Medicine Children’s Health: Mood Disorders
- Teen Line Support
- Child Mind Institute: How Anxiety Affects Teens
- Psychology Today: Understanding Childhood Dysregulation Profile
- Anxiety and Depression Association of America: Anxiety Disorders